Treatment of GIST
GIST appears in different forms which range from small, almost unnoticeable 1-2 cm tumors to big, well isolated, operable tumors to bloody tissue proliferation and metastases that run through the abdominal tissue like pearls. All GIST are malignant and have the potential to spread among the whole body.
In general: Early discovery and professional treatment and management usually leads to better outcomes and improved prognosis.
There are the three stages of the disease:
- Locally isolated, operable primary tumor (no metastases)
- Inoperable / metastasized (advanced) GIST
- Progression = development of the metastasized disease under therapy
Treatment strategy should be discussed in a multidisciplinary team including pathologists, radiologists, surgeons, and medical oncologists, as well as gastroenterologists, nuclear medicine specialists etc., if applicable. It depends on the stage of the disease, localization of the tumor and its metastasis, gene mutations and general state of health of the patient.
Especially in small GIST, complete removal is the standard treatment, unless major morbidity is 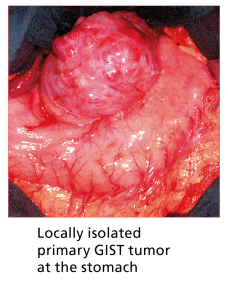 expected. The so called R0 resection (complete removal of the tumor) is an important factor for prognosis. Therefore, operable tumors should always be removed by surgery if a complete resection seems possible.
expected. The so called R0 resection (complete removal of the tumor) is an important factor for prognosis. Therefore, operable tumors should always be removed by surgery if a complete resection seems possible.
Risk of relapse and the question of adjuvant treatment
There is a significant risk of relapse: more than half of all patients experience a recurrence (= relapse) or a development of metastasis after complete resection. That is why a risk stratification is done to determine whether a preventative (= adjuvant) drug therapy and/or long-term follow-up with short time intervals is indicated.
Risk Stratification: A number of factors are thought to lead to recurrence. The current method for assessing the probability of relapse is a risk classification by the American pathologist Miettinen, created in 2006. It assesses tumour size, the rate of cell division (= mitotic rate/mitotic count) but also the location of the tumour.
The decision whether or not a patient needs to receive a preventative (=adjuvant) drug-based treatment depends on the outcomes of the risk classification. Patients with a high risk of relapse should always receive adjuvant treatment whereas patients with low risk shouldn’t receive medication. In patients with intermediate risk, the decision needs to be taken individually.
The objective of such a treatment strategy is to lower this risk of relapse and to support the effects of the surgery as primary therapy. It aims to eliminate possible existing tumor cells not yet visible or measurable, or micro-metastases.
Currently, only one drug is approved for post-operative, adjuvant treatment: Imatinib (Gleevec®/Glivec®).
Neoadjuvant treatment
Imatinib can also be administered in the so-called neoadjuvant setting. That means the drug is given before surgery is done.
This is usually done:
- in large, seemingly inoperable tumors
- if patients would need to undergo extensive (wide-ranging, severe) surgery with possibly serious post-operative complications
Neoadjuvant treatment is applied in order to improve the initial situation for the surgery: It should make the tumor operable and/or possibly minimize the scope of the operation. It should be given at least 4 to 6 months in order to reach "maximum response", which is the optimal moment for surgery. It is worth noting that a good proportion of such patients benefit from this type of treatment, with the result that the surgery is far less extensive than originally expected.
{slider Metastatic GIST|blue}
Until the year 2000, the only way to treat even advanced cancers was surgery (= resection.) As GIST proved very resistant to both traditional chemotherapy and radiation, it used to be very difficult to treat: The average time of survival with a metastasized disease was 12 months.
 In 2002, Imatinib (Gleevec®/Glivec®) was approved for treatment of c-Kit (CD117)-positive unresectable and/or metastatic GIST in adults. It is the first marketed “molecularly targeted therapy” for cancer. This means that the drug affects only those cells that express highly specific targets, in contrast to conventional cancer chemotherapies that affect all fast-growing cells in the body. The targets of imatinib in GIST patients are two growth-factor receptors named KIT and PDGFRA. In 90-95 % out of all GIST patients, mutations in one of these genes can be detected. These mutations are responsible for uncontrolled cell division leading to cancer. Imatinib targets those mutations and thus stops the tumor growth.
In 2002, Imatinib (Gleevec®/Glivec®) was approved for treatment of c-Kit (CD117)-positive unresectable and/or metastatic GIST in adults. It is the first marketed “molecularly targeted therapy” for cancer. This means that the drug affects only those cells that express highly specific targets, in contrast to conventional cancer chemotherapies that affect all fast-growing cells in the body. The targets of imatinib in GIST patients are two growth-factor receptors named KIT and PDGFRA. In 90-95 % out of all GIST patients, mutations in one of these genes can be detected. These mutations are responsible for uncontrolled cell division leading to cancer. Imatinib targets those mutations and thus stops the tumor growth.
Imatinib in the dosage of 400 mg/day (to 800 mg/day in specific cases) is standard in first-line therapy and should be started straight after confirmed diagnosis of metastatic and/or unrespectable GIST. Due to high effectiveness and good tolerability, it can contribute to a significant increase in life expectancy and quality of life.
Whether or not a patient is likely to respond to a certain drug therapy significantly depends on the mutation of the primary tumour. Again, mutation analysis therefore is extremely important.
| Imatinib | Sunitinib | |
| KIT | ||
| Exon 9 | 800 mg | Good |
| Exon 11 | Good | Bad |
| PDGFR | ||
| Exon 12 | Good | No data |
| Exon 18 (without D842V) | Good? | No data |
| Exon 18 (D842V) | No | No |
| Exon 18 (D842Y) | Good (Lab) | No data |
| Wild type GIST | ||
| Bad to satisfactory | Good |
To date, the value of surgery of metastasis in a metastatic situation and under drug therapy is still unclear: There is no data about a possible advantages or disadvantages from this intervention. This needs to be evaluated in clinical trials.
{slider Disease Progression during drug therapy|blue}
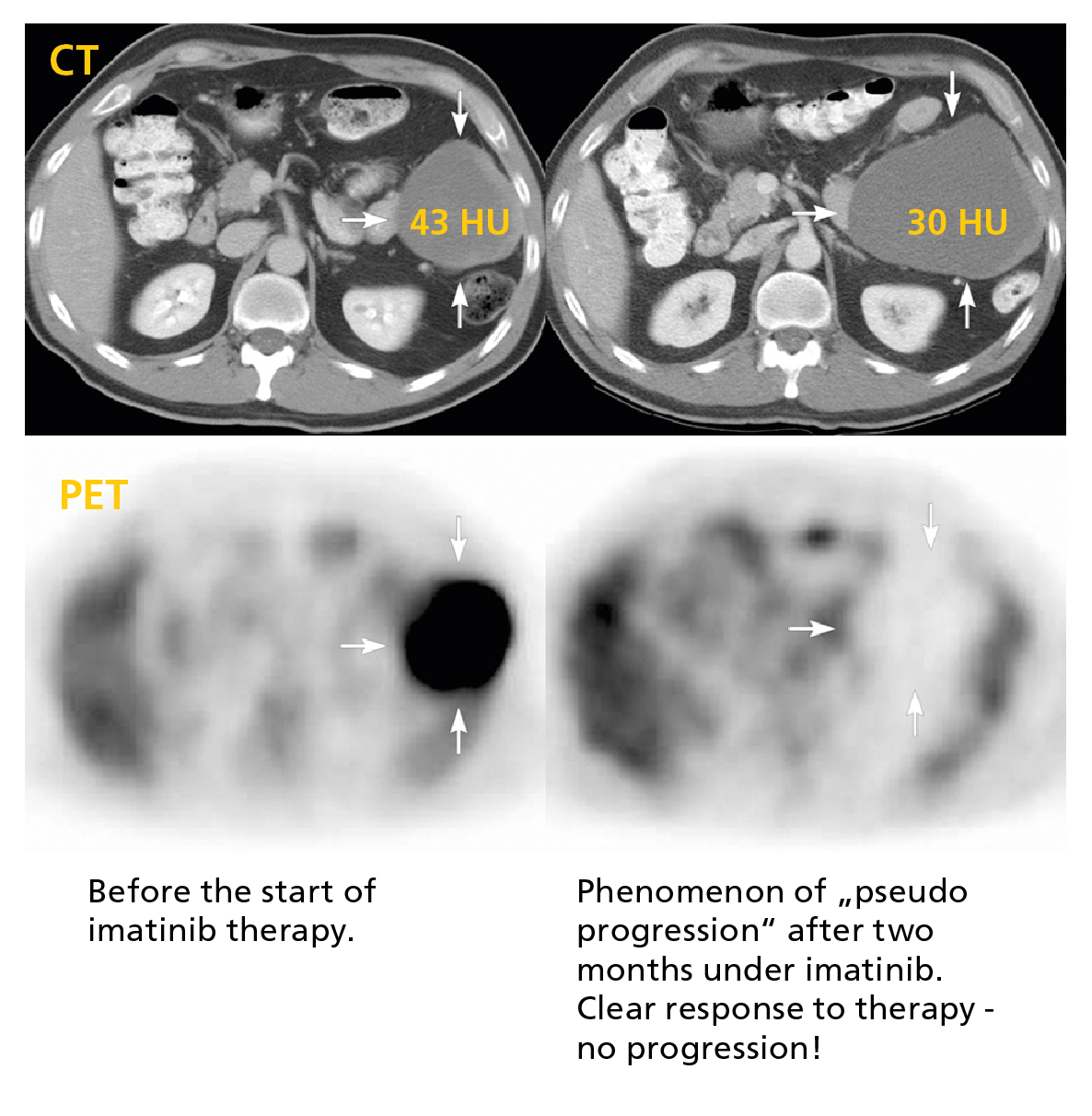
Despite the high effectiveness of imatinib in GIST, disease progression after two or three years is unfortunately observed in a significant proportion of patients. It is called imatinib resistance.
When this happens, certain measures have to be taken:
- Verify that this a definite disease progression and exclude other reasons e.g. compliance issues, interaction with other medications etc.
- Clarify, if it is happening in several locations (= systemic) or only at the original site of the tumor (= localised).
Before switching therapies, further options of localised treatments should be evaluated. Such treatments include Radio Frequency Ablation (RFA), Laser Induced Interstitial Thermotherapy (LITT) and Selective Internal Radiation Therapy (SIRT). Since therapy options are still limited, it is vital to make sure that patients benefit from any therapy for as long as possible with an acceptable quality of life.
If progression is confirmed, there are different options:
- Experienced GIST experts can suggest an individualised treatment plan, e.g. if the progression is very slow. In this case, a "wait & watch" approach can be an option. This means closely monitoring the progressing disease until a change in therapy is necessary, or new options arise from clinical studies.
- Dose escalation of Imatinib: Usually the first step after confirmed progression is to raise the dose of Imatinib to 800 mg/day. Approximately one third of all patients show a response again.
- In case of Imatinib resistance (or intolerance) the multikinase inhibitor Sunitinib (Sutent®) offers another, effective means of therapy. In contrast to Imatinib - a continuous therapy - Sunitinib is a cycle therapy with a 6-week-cycle (4 weeks of therapy, followed by 2 weeks break) administered at a dose of 50 mg/day. In clinical practice, however, a continuous therapy (with no breaks) is also used with a dosage of 37.5 mg/day. GIST patients with a primary mutation in Exon 9, or with no indication of mutation (wild type) can benefit from Sunitinib for a longer period of time.
- Regorafenib/Stivarga® has been approved in several countries for the treatment of patients with unresectable metastatic GIST that no longer respond to Imatinib and Sunitinib. The standard dose for Stivarga is 160 mg for 3 weeks followed by 1 week without drug.
- If progression continues, many GIST experts currently recommend two further substances (Nilotinib/Tasigna® and Sorafenib/Nexavar®), even though they are not approved for the treatment of GIST. This type of use is termed “off-label use”. However, they have shown to be effective in GIST in clinical trials. The administration of such off-label therapies requires an agreement (consent) between the attending doctor and the relevant health insurance.
- Inclusion in clinical trials.
Please find below an overview of approved targeted therapies in GIST:
